Monitoring preservation's transition from the laboratory into clinical practice — through rigorous, provider-neutral quality standards and independent assessment.
The potential of preserving people for possible future revival depends on maintaining the neural structures that encode memories, personality, and identity. Ensuring preservation procedures actually achieve this requires rigorous assessment standards to verify that critical brain structures remain intact. Historically there have been no standardized quality metrics or independent third-party evaluation of preservation providers, making it difficult for patients to assess different procedures or for the field to demonstrate scientific legitimacy. To address this, the Brain Preservation Foundation intends to establish quality standards and an accreditation program: independent assessment of preservation providers to improve technical rigor, encourage best practices, and help transition high-quality brain preservation from research into credible clinical practice.
The foundational premise of brain preservation for life extension is that by preventing a brain from decaying — stabilising the neural structures that underlie someone's memories, personality, and psychological properties — the potential remains for that person to one day be revived. As in deep anaesthesia or induced hypothermia, where patients undergo complete but reversible cessation of brain activity, individuals may be able to survive indefinite periods of stasis, so long as their brains are preserved sufficiently well.
Current neuroscientific consensus holds that long-term information in human brains is stored primarily in the pattern of synaptic connections between neurons, which in turn depend on properties such as receptor types and densities, axonal myelination, perineuronal-net modifications, and other molecular and structural features. In 2010 the BPF established a prize for the first team to preserve an entire brain "with such fidelity that the structure of every neuronal process and every synaptic connection remains intact and traceable using today's electron microscopic imaging techniques." That prize was won in 2018 with aldehyde-stabilized cryopreservation (ASC), demonstrating that this concrete benchmark can be met.
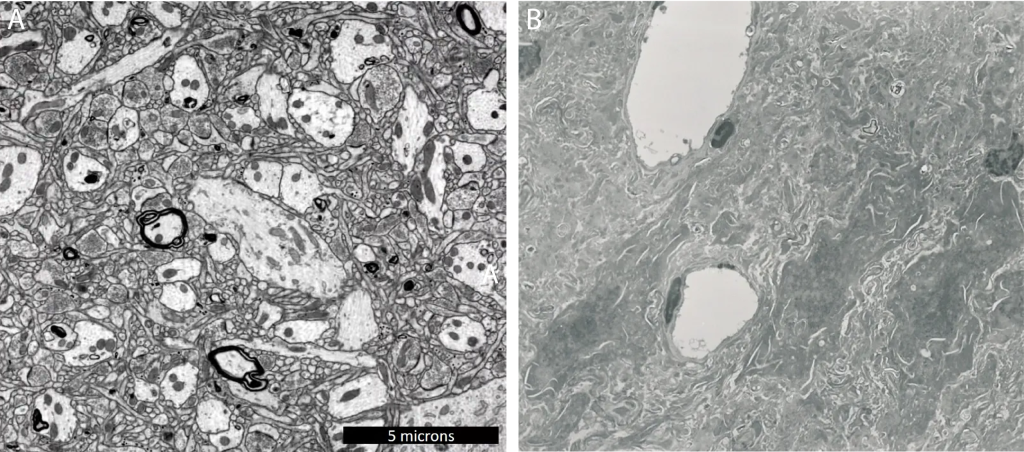
In contrast, historical attempts to preserve patients for future revival have not met this minimum standard. Traditional cryopreservation of human patients has resulted in severe dehydration and brain shrinkage of 30–50%, leaving tissue highly compressed and structurally abnormal under electron microscopy. While it is conceivable that such shrinkage could occur while preserving connectivity information, it is equally plausible that it masks osmotic and ischemic damage. This unclear quality is a barrier for patients, and the lack of standardized metrics makes it hard for providers to improve or for the wider community to evaluate the field's legitimacy.
These standards are meant to be generic across all preservation protocols — fixative, cryopreservative, or as-yet undiscovered — and will evolve as methods, readouts, and our understanding of neurophysiological information storage develop. They assume a brain that was structurally intact with minimal damage prior to the procedure, an assumption that may be violated in clinical settings (e.g. prolonged agonal hypoxia, or advanced dementia).
Providers submit a comprehensive protocol including: detailed preservation procedures; critical steps and their plausible failure modes; per-case quality-assessment methods; non-destructive evaluation steps that verify preservation quality; and documentation of equipment, training, and facility requirements.
After approval, providers demonstrate effectiveness through controlled testing using either animal models (typically large mammals such as pigs) or human research donations with specific consent for destructive full-brain evaluation. This phase proves that the proposed non-destructive methods can reliably assess quality, with consistent results across multiple test cases required before accreditation.
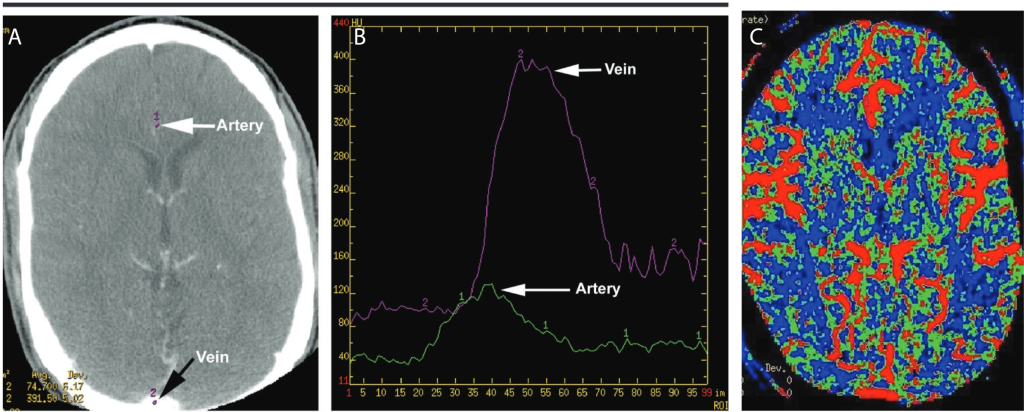
Only after successful validation may providers offer accredited procedures to patients. All accredited human cases must be pre-registered with the BPF (allowing for emergency exceptions), conducted to the approved protocol, and documented with complete quality evaluation — including at least one non-destructive method to assess perfusion of all brain regions (e.g. CT perfusion, X-ray angiography, perfusion MRI) and at least one minimally-invasive method to assess ultrastructure (e.g. small punch biopsies analysed by electron or expansion microscopy).
Each pre-registered, anonymised case will be listed on a dedicated BPF registry and followed to completion, with all evaluations and outcomes posted publicly. Where a case fails to meet the standards, the BPF will document the specific deficiencies and may require additional validation testing before future cases, or revoke accreditation.
We invite preservation providers committed to rigorous scientific standards to engage with this process, and we welcome researchers, clinicians, bioethicists, funders, and policymakers who recognise the importance of proper oversight for this emerging field. To support this work through funding or technical expertise, please reach out at standards@brainpreservation.org.